Redetermination Form For Medicare - Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Get forms to appeal a medicare coverage or payment decision. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Your next level of appeal is a. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal.
Get forms to appeal a medicare coverage or payment decision. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Your next level of appeal is a. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or.
Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Get forms to appeal a medicare coverage or payment decision. Your next level of appeal is a. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or.
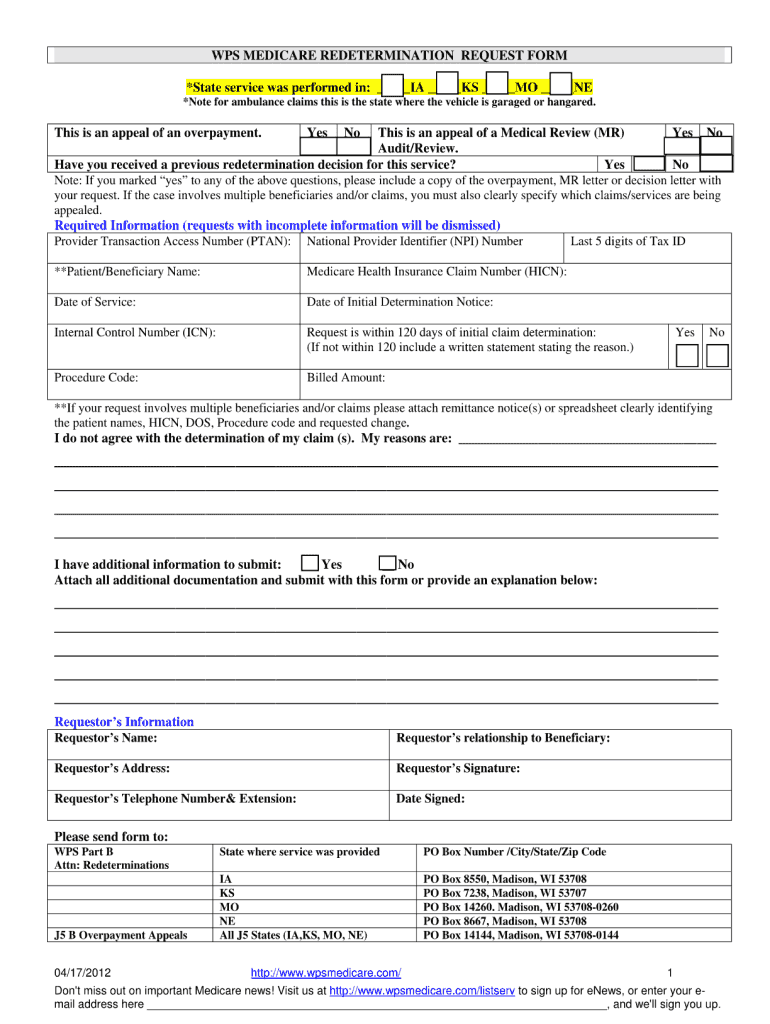
Form Cms20027 Medicare Redetermination Request Form, Form Cms20034
Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Your next level of appeal is a. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. If you received a medicare redetermination notice (mrn) on this.

Fillable Online Medicare Redetermination Form Step By Step Fax Email
Your next level of appeal is a. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Get forms to appeal a medicare coverage or payment decision. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit.

Fillable Online Part A Redetermination Request Form. Part A
Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Get forms to appeal a medicare coverage or payment decision. Your next level of appeal is a. Please attach the evidence.
Fillable Form Mc 262 Redetermination For MediCal Beneficiaries (Long
Get forms to appeal a medicare coverage or payment decision. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Your next level of appeal is a. Please attach the evidence.
Fillable Online Reqest for redetermination of Medicare Prescription
Get forms to appeal a medicare coverage or payment decision. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice.
Medicare dme redetermination request form Fill out & sign online DocHub
Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Your next level of appeal is a. Get forms to appeal a medicare coverage or payment decision..
Medicare redetermination form Fill out & sign online DocHub
Get forms to appeal a medicare coverage or payment decision. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. If you received a medicare redetermination notice.
Redetermination Cook County Health
Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or. Your next level of appeal is a. If you received a medicare redetermination notice (mrn) on this.

Medicare Part B JF Redetermination Form PDF
Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Your next level of appeal is a. Get forms to appeal a medicare coverage or payment.

20202025 CMS Medicare DME Redetermination Request Form Fill Online
Get forms to appeal a medicare coverage or payment decision. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Anyone who misrepresents or falsifies essential.
Anyone Who Misrepresents Or Falsifies Essential Information Requested By This Form May Upon Conviction Be Subject To Fine Or.
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Get forms to appeal a medicare coverage or payment decision. Your next level of appeal is a.