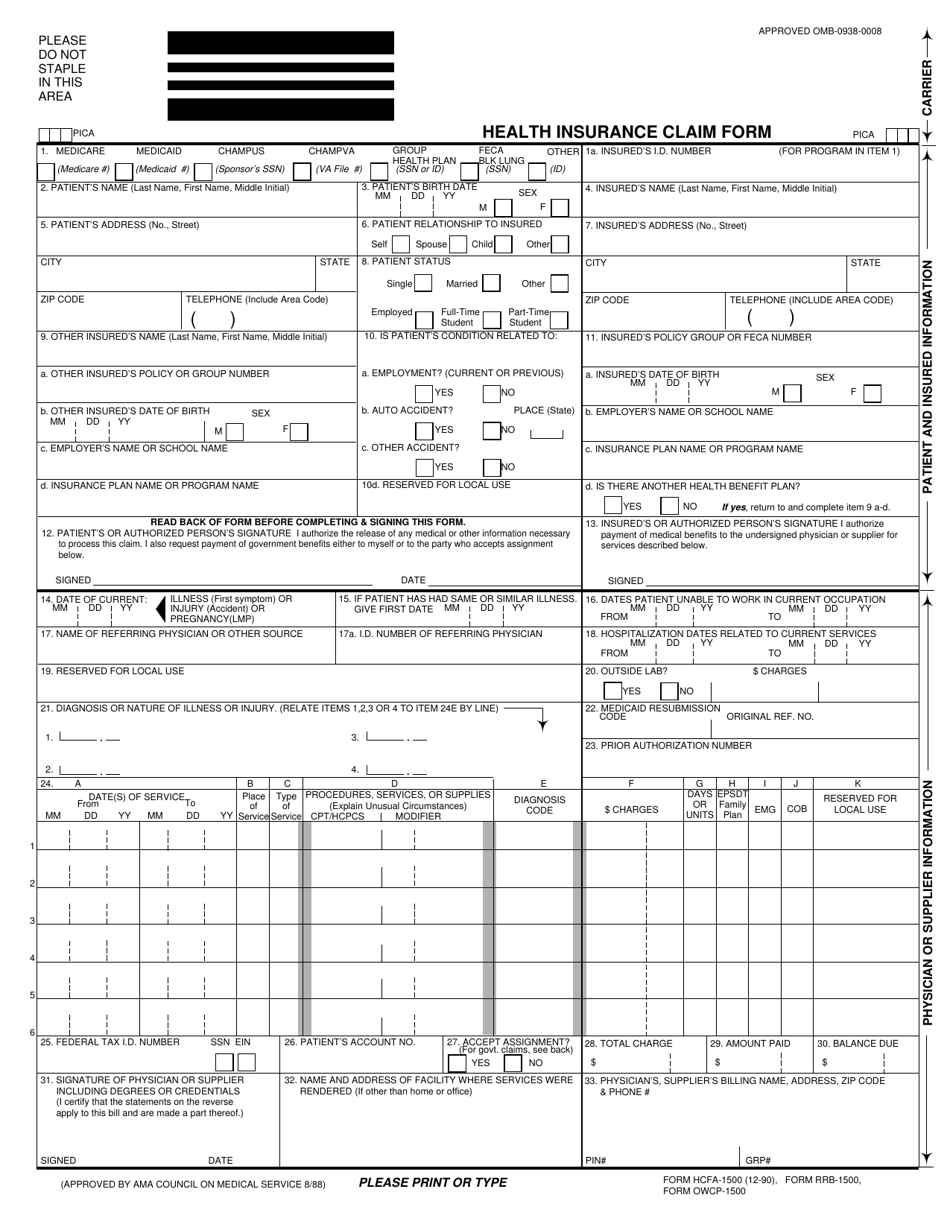
Hcfa 1500 Claim Form - Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. It is the basic paper claim form prescribed. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. The cms 1500 claim form is the uniform or standard claim form used by a provider or supplier to bill and dmercs (durable medical. If errors are detected at this. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard.
The cms 1500 claim form is the uniform or standard claim form used by a provider or supplier to bill and dmercs (durable medical. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard. It is the basic paper claim form prescribed. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. If errors are detected at this.
If errors are detected at this. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. The cms 1500 claim form is the uniform or standard claim form used by a provider or supplier to bill and dmercs (durable medical. It is the basic paper claim form prescribed. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim.

Hcfa 1500 Form Printable
Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. The 1500 health insurance claim form (1500 claim form) answers the needs of many health.

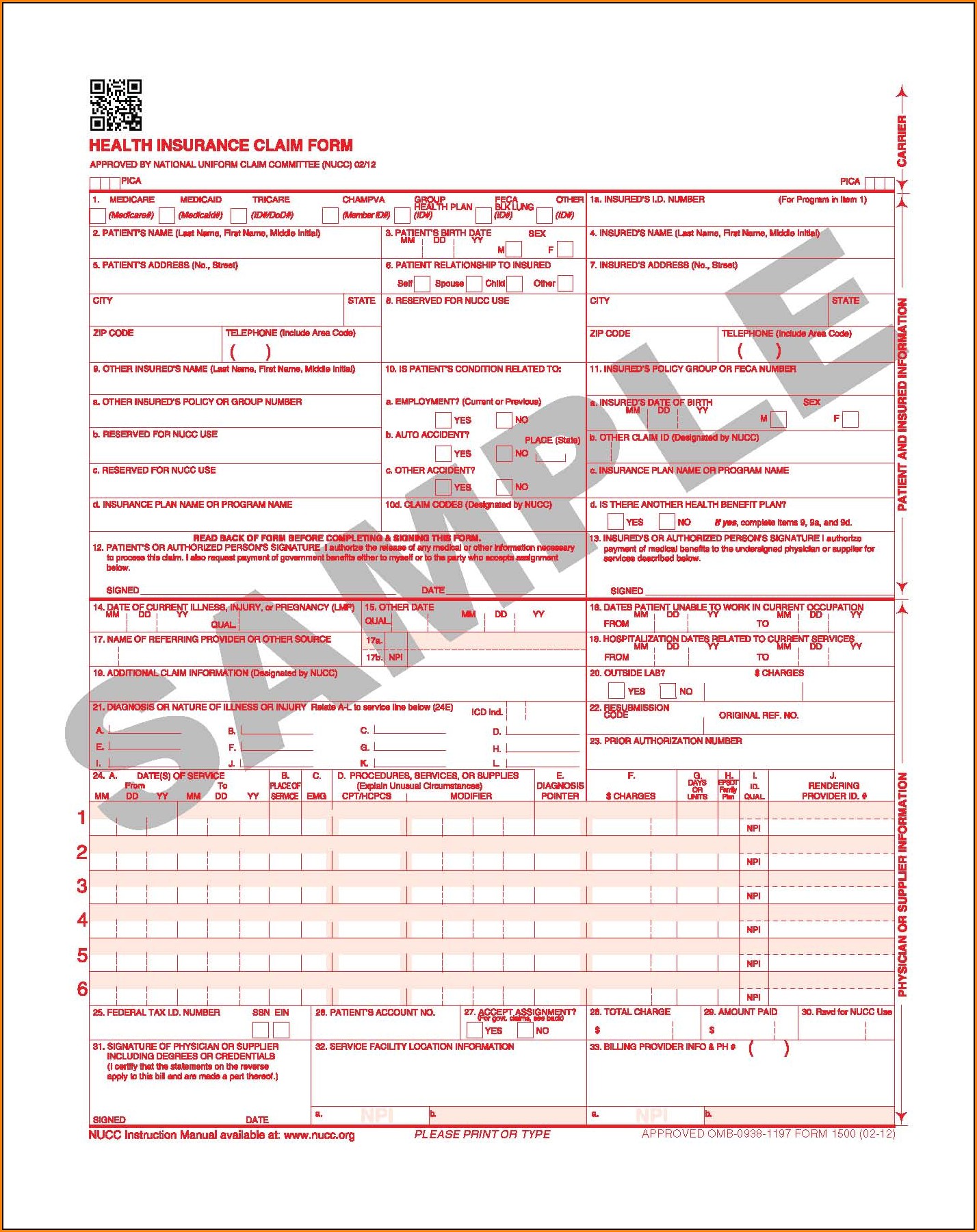
CMS 1500 Claim Forms HCFA (Version 02/12) 2,500 SHEETS
If errors are detected at this. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. The 1500 health insurance claim form (1500 claim form).

Printable Fillable Hcfa 1500 Claim Form Printable For vrogue.co
If errors are detected at this. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. I understand that payment and satisfaction of this claim will be from federal and state funds, and.
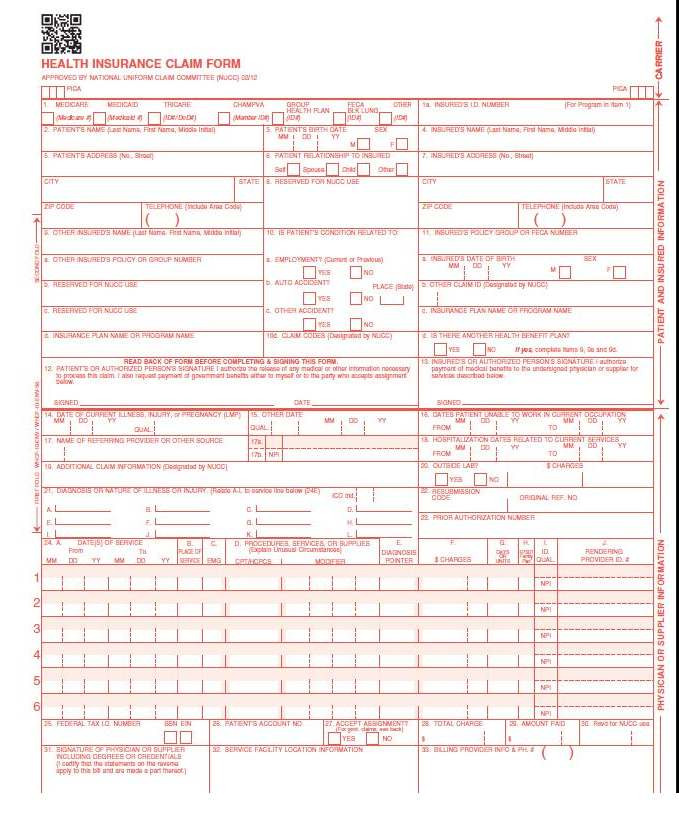
Form HCFA1500 Fill Out, Sign Online and Download Printable PDF
The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. If errors are.
Printable Hcfa 1500 Claim Form Hcfa 1500 Cms Form Forms Clai
It is the basic paper claim form prescribed. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. Patient’s or authorized person’s signature i authorize the release of.
Hcfa 1500 Claim Form Printable Form Resume Examples P32ERx49J8
It is the basic paper claim form prescribed. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. If errors are detected at this. The initial edits are.

Printable Fillable Hcfa 1500 Claim Form Printable Forms Free Online
The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. If errors are detected at this. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. The initial edits are to determine if the claims in a batch.

Sample Completed Hcfa 1500 Form
It is the basic paper claim form prescribed. The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or. The 1500 health insurance claim form (1500.

Printable Hcfa 1500 Claim Form Form Resume Examples ygKzkewV3P
If errors are detected at this. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. The cms 1500 claim form is the uniform or standard claim form used by a provider or supplier to bill and dmercs (durable medical. Patient’s or authorized person’s signature i authorize the release of any medical or.
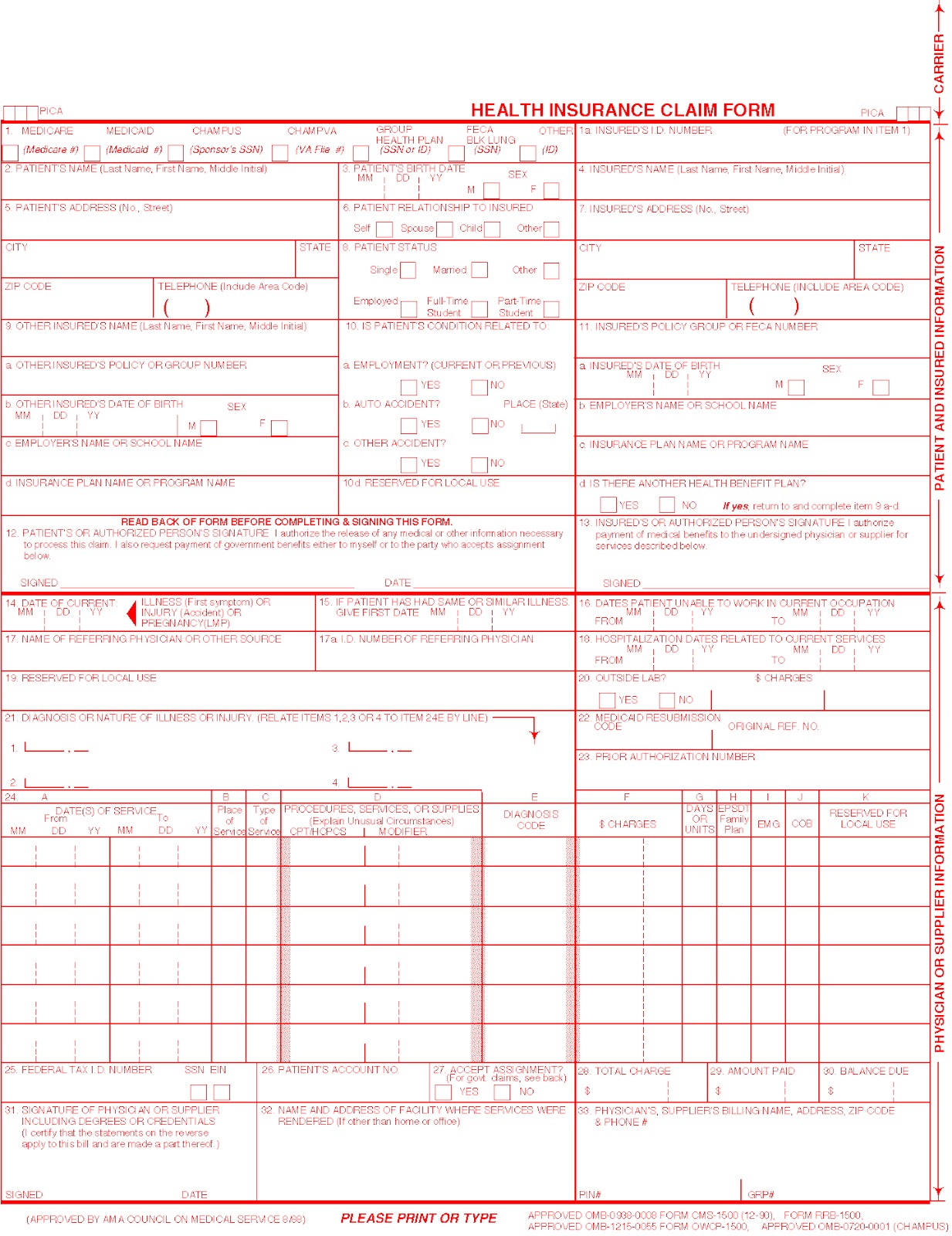
Printable Hcfa 1500 Form
If errors are detected at this. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard. The cms 1500 claim form is the uniform or standard claim form used by.
The Cms 1500 Claim Form Is The Uniform Or Standard Claim Form Used By A Provider Or Supplier To Bill And Dmercs (Durable Medical.
The initial edits are to determine if the claims in a batch meet the basic requirements of the hipaa standard. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. If errors are detected at this. I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, or documents, or.
The 1500 Health Insurance Claim Form (1500 Claim Form) Answers The Needs Of Many Health Care Payers.
It is the basic paper claim form prescribed.