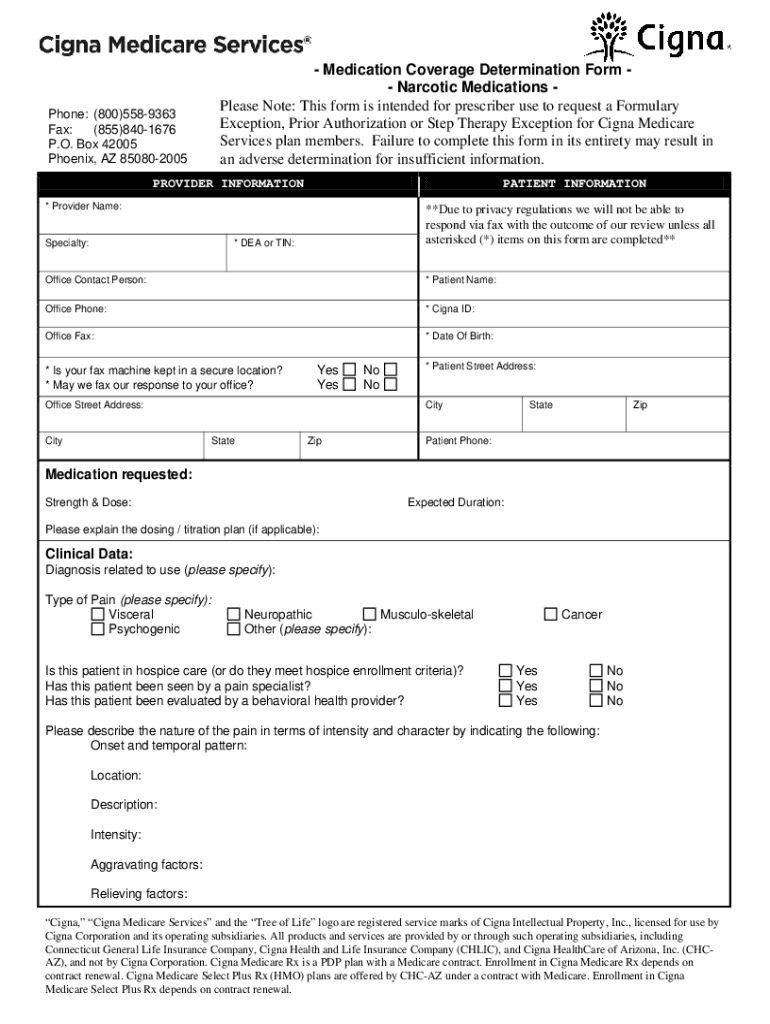
Formulary Exception Form - Benefits for services received are subject to eligibility and. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Before completing this form, please confirm the patient’s benefits and eligibility.
A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Before completing this form, please confirm the patient’s benefits and eligibility. Benefits for services received are subject to eligibility and. Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug.
Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Benefits for services received are subject to eligibility and. Before completing this form, please confirm the patient’s benefits and eligibility. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to.

Formulary Exception Form Fill Online, Printable, Fillable, Blank
A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Benefits for services received are subject to eligibility and. Before completing this.
Fillable Online Pharmacy Formulary Exception Process/Prior
Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Benefits for services received are subject to eligibility and. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Before completing this.

Sunlife Drug Exception Form Fill Out And Sign Printable PDF Template
A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Before completing this form, please confirm the patient’s benefits and eligibility. Benefits.
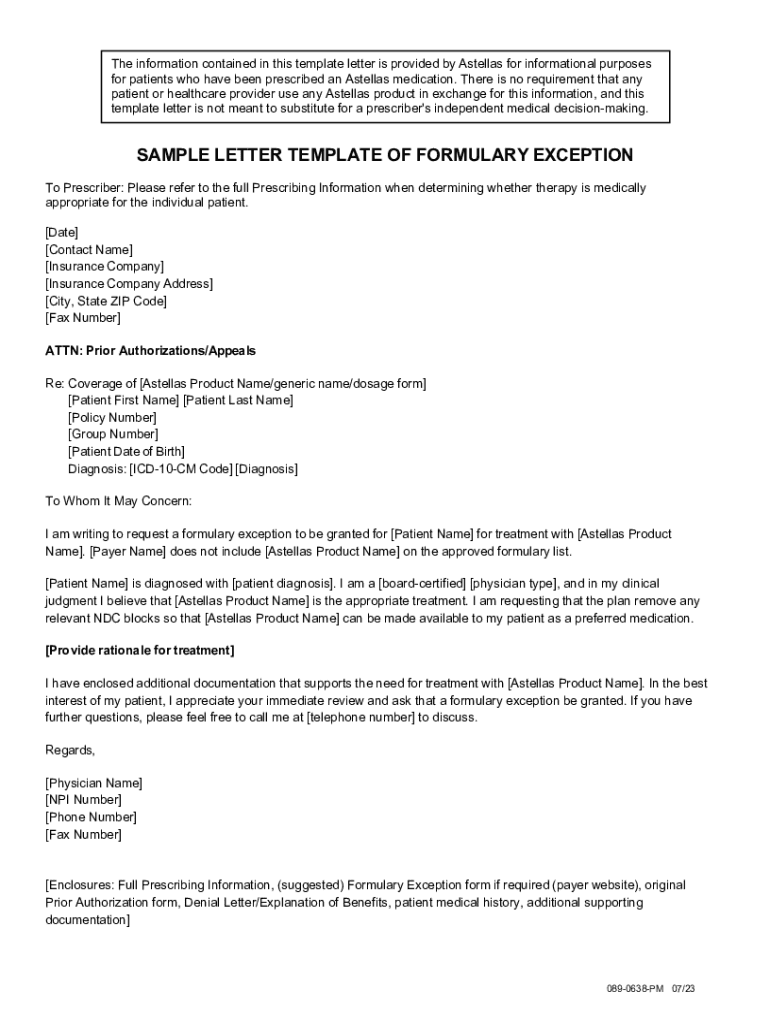
Fillable Online SAMPLE LETTER TEMPLATE OF FORMULARY EXCEPTION Fax Email
Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Benefits for services received are subject to eligibility and. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Before completing this.
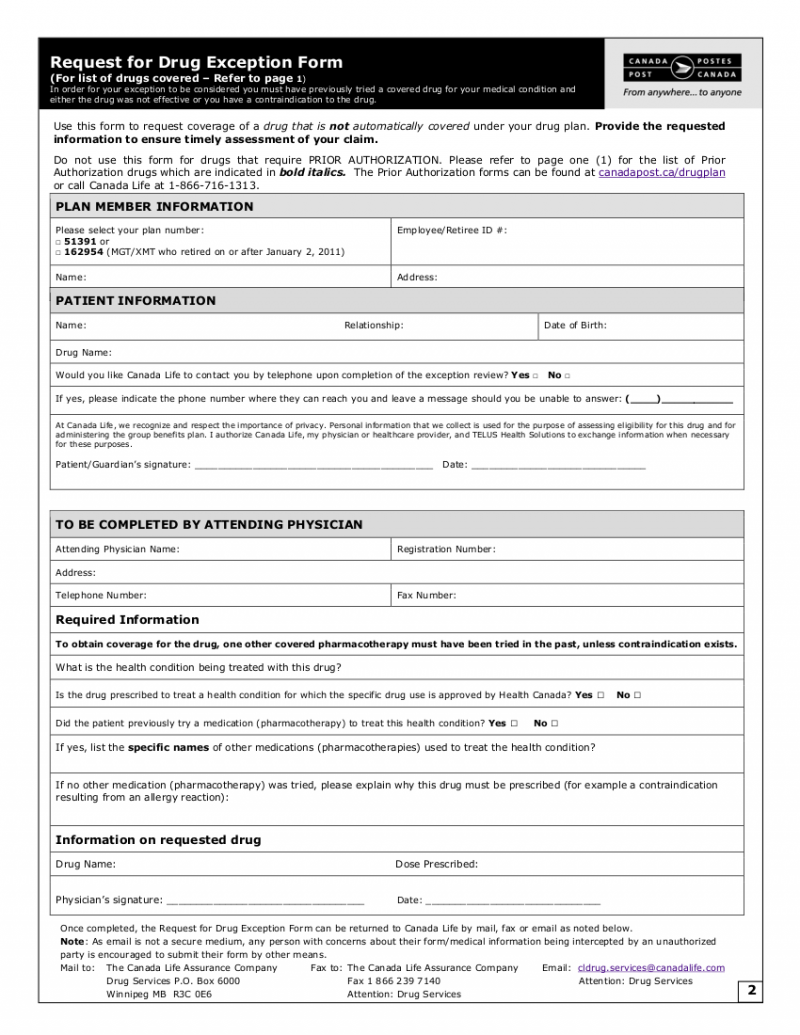
List of Covered Drugs and Request for Drug Exception Form CUPW
Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Benefits for services received are subject to eligibility and. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Before completing this.

Bcbs Exception Prior Request Form Fill Online, Printable, Fillable
Before completing this form, please confirm the patient’s benefits and eligibility. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Benefits for services received are subject to eligibility and. Does the patient have a clinical condition for which other formulary alternatives are not recommended.
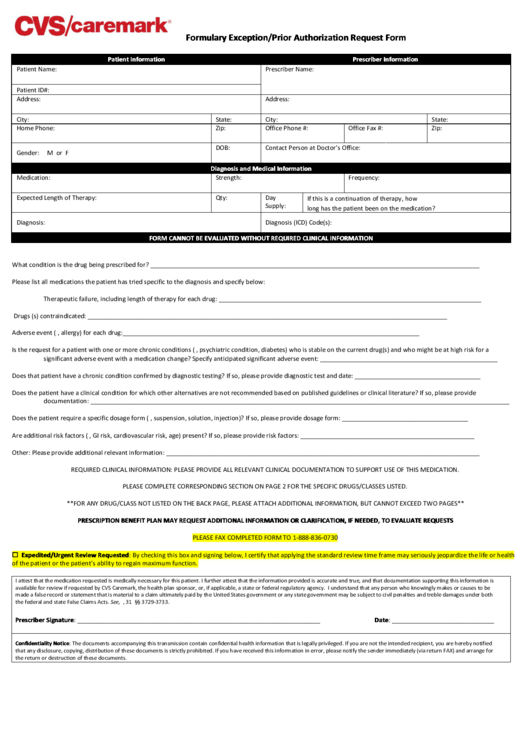
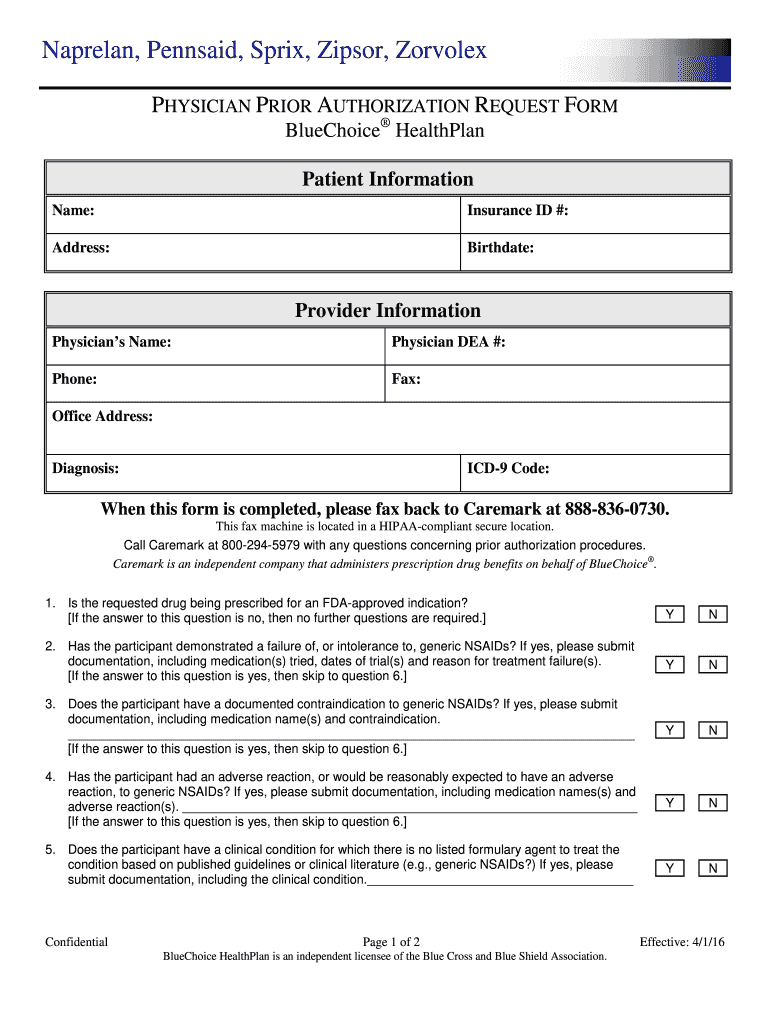
Formulary Exception/prior Authorization Request Form printable pdf download
Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Benefits for services received are subject to eligibility and. Before completing this.
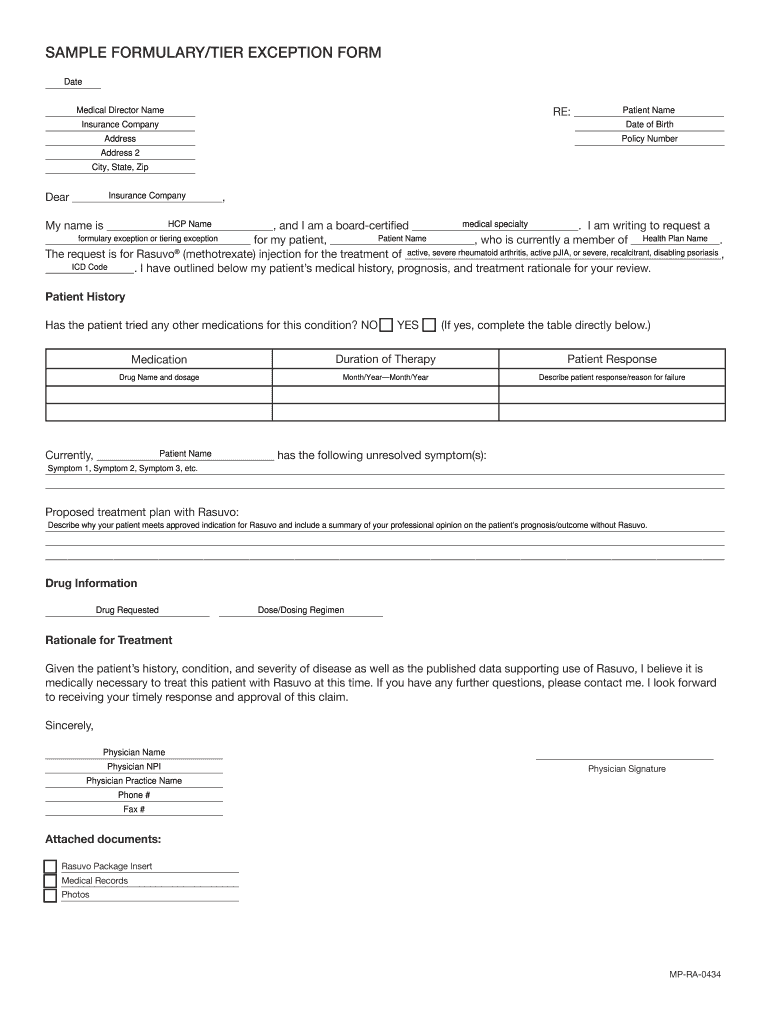
Fillable Online SAMPLE FORMULARY/TIER EXCEPTION FORM Fax Email Print
Before completing this form, please confirm the patient’s benefits and eligibility. Benefits for services received are subject to eligibility and. Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. A formulary exception should be requested to obtain a part d drug that is not included on.
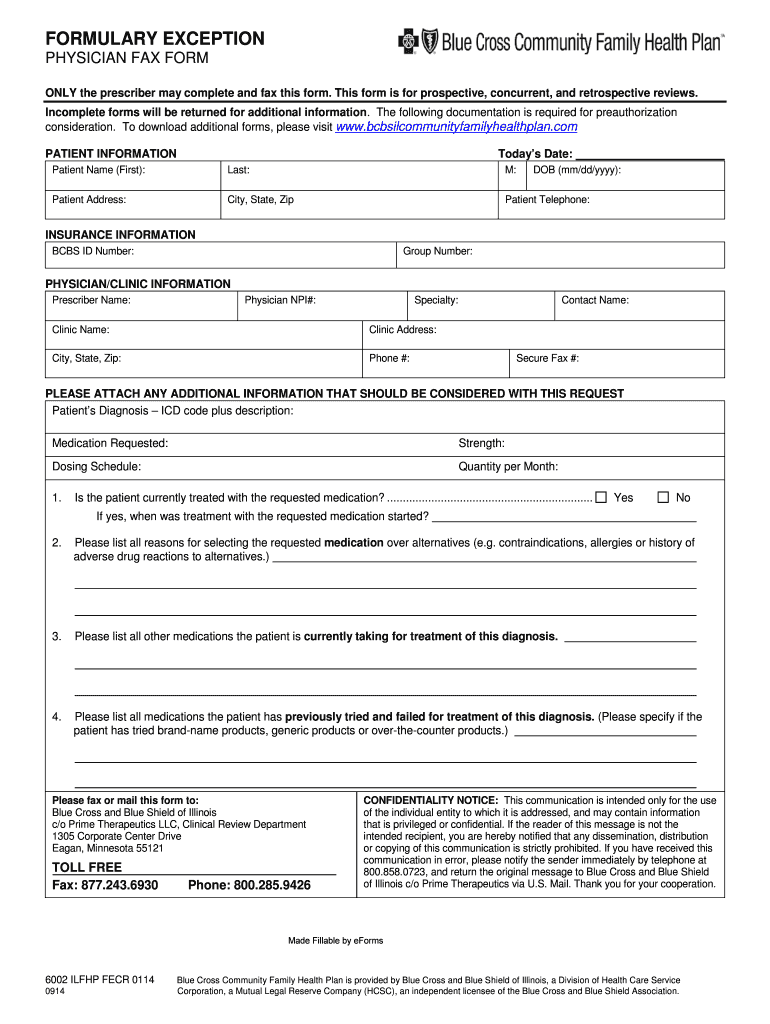
FORMULARY EXCEPTION PHYSICIAN FAX FORM Fill Out and Sign Printable
Before completing this form, please confirm the patient’s benefits and eligibility. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. Benefits.
Caremark Formulary Exception Form Fill Online, Printable, Fillable
A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Benefits for services received are subject to eligibility and. Before completing this form, please confirm the patient’s benefits and eligibility. Does the patient have a clinical condition for which other formulary alternatives are not recommended.
Benefits For Services Received Are Subject To Eligibility And.
Does the patient have a clinical condition for which other formulary alternatives are not recommended or are contraindicated due to comorbidities or drug. A formulary exception should be requested to obtain a part d drug that is not included on a plan sponsor's formulary, or to request to. Before completing this form, please confirm the patient’s benefits and eligibility.