Bcbs Dispute Form - Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. Physicians and providers may request reconsideration of how a claim processed, paid or denied. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: These requests are referred to as appeals. The most commonly used physician and provider forms are. Forms for florida blue members enrolled in individual, family and employer plans.
These requests are referred to as appeals. Forms for florida blue members enrolled in individual, family and employer plans. Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. The most commonly used physician and provider forms are. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Physicians and providers may request reconsideration of how a claim processed, paid or denied.
The most commonly used physician and provider forms are. These requests are referred to as appeals. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. Physicians and providers may request reconsideration of how a claim processed, paid or denied. Forms for florida blue members enrolled in individual, family and employer plans.

Fillable Online Member Appeal Request Form BCBSTX Fax Email Print
Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Forms for florida blue members enrolled in individual, family and employer plans. The most commonly used physician and provider forms are. Providers serving members in the state of illinois may use this form to request information about claim status.

Fillable Online Medicare Advantage Provider Appeal Form Fax Email Print
Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Forms for florida blue members enrolled in individual, family and employer plans. These requests are referred to as appeals. Providers serving members in the state of illinois may use this form to request information about claim status or dispute.
Nalc Health Benefit Plan Provider Appeal Form
These requests are referred to as appeals. Forms for florida blue members enrolled in individual, family and employer plans. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Providers serving members in the state of illinois may use this form to request information about claim status or dispute.
Highmark bcbs pa provider appeal form Fill out & sign online DocHub
These requests are referred to as appeals. Forms for florida blue members enrolled in individual, family and employer plans. Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. Physicians and providers may request reconsideration of how a claim processed, paid or denied. The most.

Fillable Online New Provider Appeal Form Premera Blue Cross Fax Email
Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Physicians and providers may request reconsideration of how a claim processed, paid or denied. Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross..

Bcbs Prior Authorization Form Pdf Fill Out And Sign Printable PDF
Physicians and providers may request reconsideration of how a claim processed, paid or denied. Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. The most commonly used physician and provider forms are. Please describe the nature of your grievance/appeal and any facts you feel.

Bcbs Reconsideration Form Texas Fill Online, Printable, Fillable
Forms for florida blue members enrolled in individual, family and employer plans. The most commonly used physician and provider forms are. Physicians and providers may request reconsideration of how a claim processed, paid or denied. Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross..

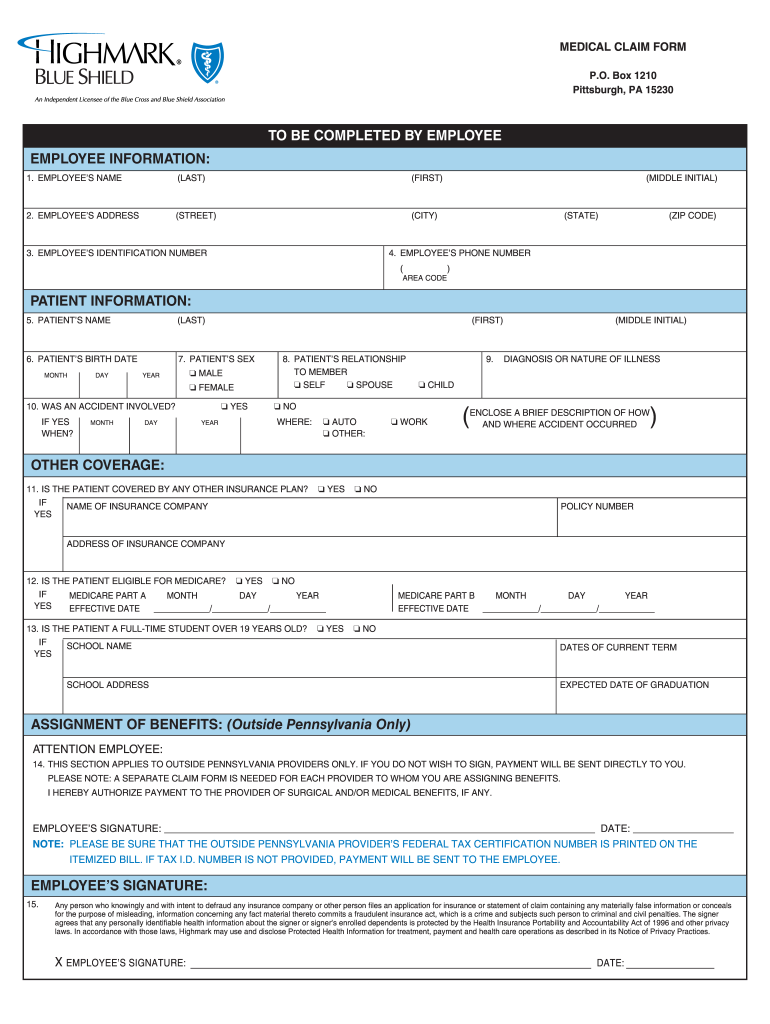
Bcbs Fep Claim Form
Forms for florida blue members enrolled in individual, family and employer plans. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: These requests are referred to as appeals. Providers serving members in the state of illinois may use this form to request information about claim status or dispute.
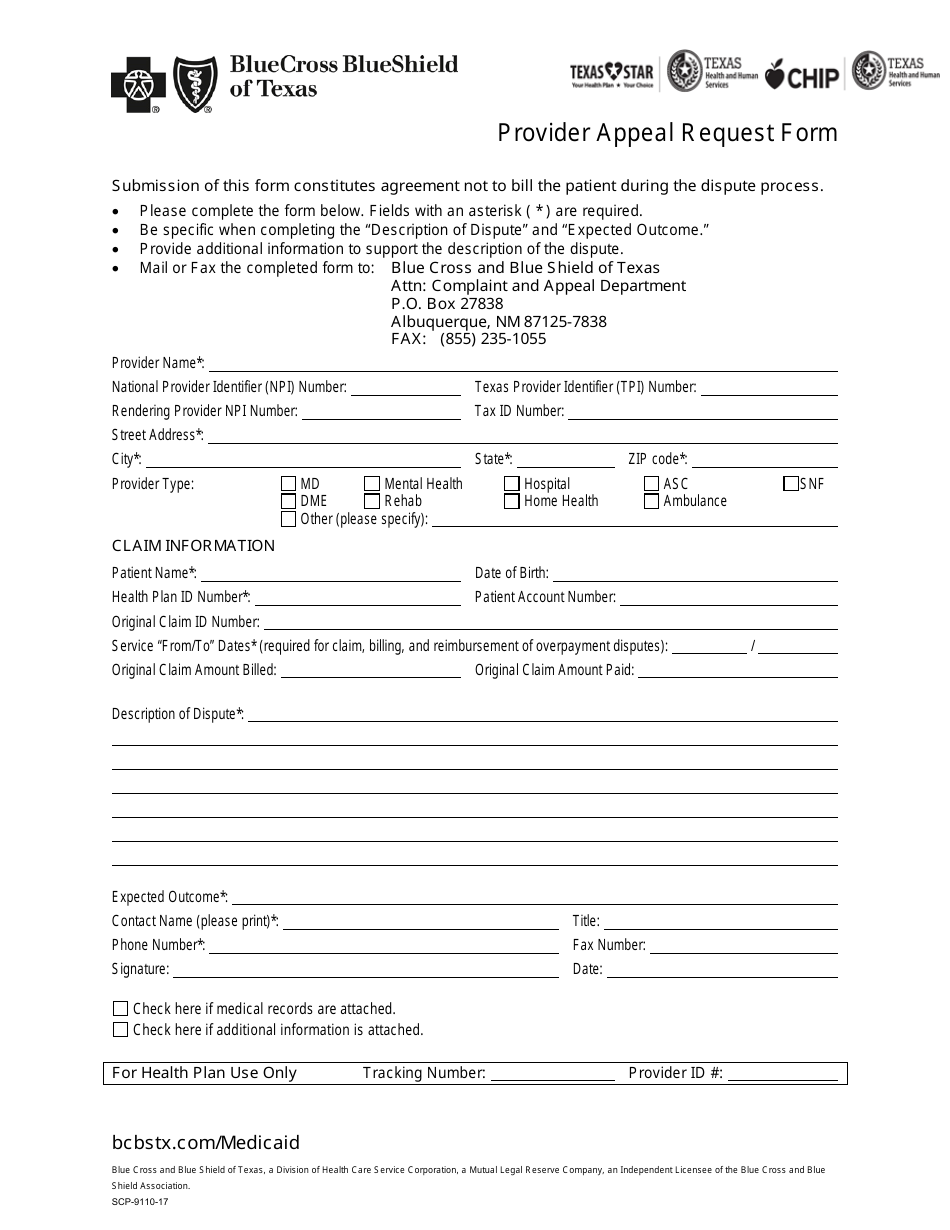
Bcbs Of Texas Appeal Form 2023 Printable Forms Free Online
These requests are referred to as appeals. Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Physicians and providers may request reconsideration of.
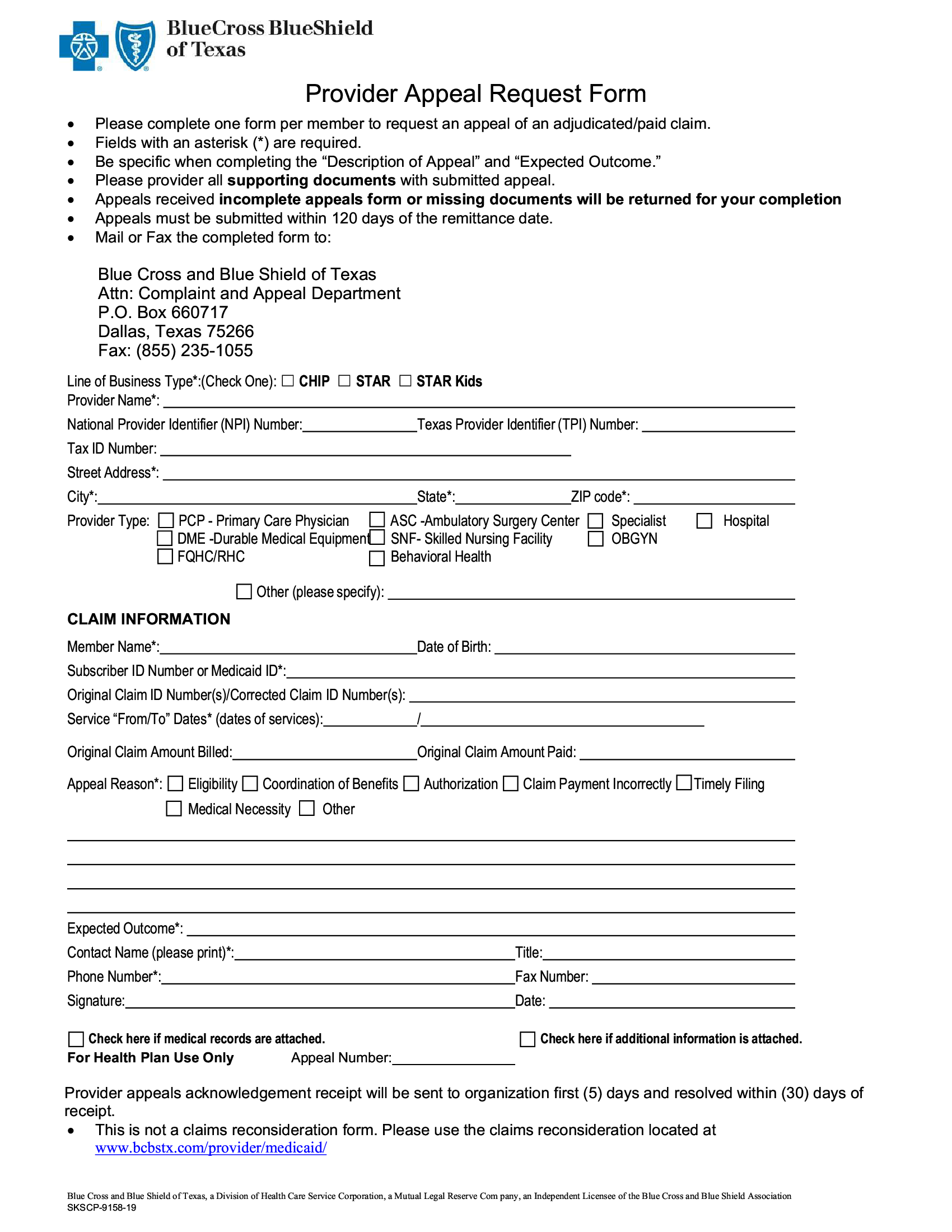
BCBS Provider Appeal Request Form Forms Docs 2023
Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Providers serving members in the state of illinois may use this form to request information about claim status or dispute a claim with blue cross. These requests are referred to as appeals. Forms for florida blue members enrolled in.
Providers Serving Members In The State Of Illinois May Use This Form To Request Information About Claim Status Or Dispute A Claim With Blue Cross.
These requests are referred to as appeals. The most commonly used physician and provider forms are. Please describe the nature of your grievance/appeal and any facts you feel should be considered in the review of your grievance/appeal: Forms for florida blue members enrolled in individual, family and employer plans.